
WHAT IS DERMATOPATHOLOGY?
Dermatopathology is the histologic study of cutaneous diseases. Cutaneous diseases are characterized by lesions, that is alterations of the skin which are readily detectable. Sometimes, a lesion is immediately identified at dermatologic visit (clinical exam), sometimes, however, clinical examination is not able to solve the problem "what is" (diagnosis). In that case, it is possible to perform a histologic exam. We can take a small amount of tissue (biopsy), which can contain the entire lesion (excisional biopsy) or only a part of it (incisional biopsy). The tissue fragment is sent to a histopathologic (from Greek, istos = tissue; pathos = disease; logos= study) laboratory in order to get a diagnosis, that is to understand what the examined lesion is. Histopatholgy studies the microscopic features of lesions of all human organs; dermatopathology, or dermatologic histopathology, studies the microscopic features of skin lesions (Greek, derma = skin). Optical microscopy (other types of microscopes do exist) is the most important tool of dermatopathologist. The removed tissue (biopsy), however, cannot be directly studied at microscope, because only histological slides can be observed at miscoscope. Therefore, it is necessary to prepare one or more slides. It is also necessary that the removed tissue fragment is not altered after the excision. Every tissue, in fact, is made by numerous cells, which are elementary living structures. Cells, when separated from the body, do alter and die. To avoid it, tissue fragments are put in a fixative solution, which (almost) instantaneously kills the cells, at the same time, mantaining them unaltered. The most used fixative is formalin (a water and formaldheid solution). After fixation, the fragment must be included in paraffin: the tissue is opportunely dehidrated and the water contained in the fragment is replaced by paraffin (at 54°C). Subsequently, a paraffin block containing the fragment to examine is made (paraffin is solid at room temperature). From the block, thin slices (sections) 0,005 mm thick are cut, using a machine called microtome. Sections are posed on a slide, deparaffined and stained with opportune stainings (at microscope without staining only cell shadows would be seen). The slide is then mounted with another thinner slide and is ready to be viewed. It is posed under the miscriscope. What one can see? One can see what there is, but can understand only what he/she knows. A slide is a piece of glass, it contains a tissue fragment, but no diagnosis. Diagnosis is a cultural elaboration. Dermatopathologist knows cutaneous lesions, interprets what he/she sees and makes a diagnosis. In conclusion, dermatopathology is the study of lesions of the skin by histology, in order to understand what type of lesion or what type of disease we are observing.
WHAT IS MELANOMA?
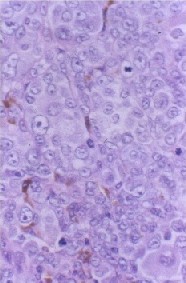
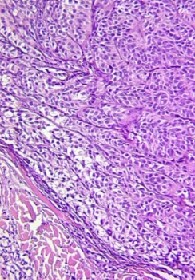
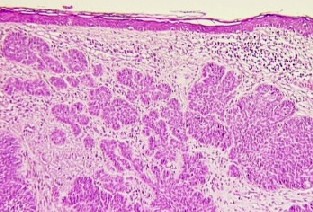
Dermatopathology studies all cutaneous lesions. Some lesions are due to inflammation (a tissue reaction against an internal or external agent) of the skin, some are malformations, some tumors (uncontrolled growth of cells, without a scope). Benign tumors are local cellular growths which push but do not destroy adjacent tissues. Malignant tumors are cellular growths, firstly local, which push and destroy adjacent tissues (infiltration) and then extend at distance (metastasis), destroying organs and tissues. In the skin, among other cells, there are some cells which form a black material called melanin: the melanocytes (Greek, melanos = black, cytos = cell). Melanocytes are located in the most superficial part of the skin (epidermis), exactly along the line (junction) which divides it from the deeper part (dermis). In the normal epidermis, there are 20 epithelial cells (keratinocytes) per 1 melanocyte. If melanocytes increase in number for some (often unknown) reasons, they may form dark cutaneous lesions (pigmented lesions). If melanocytes increase in number at the junction as single units, they form a lentigo (simplex lentigo). If they increase forming groups of cells (nests), they form a nevus or mole. The nevus is junctional, if the proliferating cells are confined to the dermoepidermal junction; it is compound, if some melanocytes are located deeper, in the dermis; it is dermal or intradermal, if all melanocytes are in the dermis. All nevi are benign: they arise in an age of the life, enlarge for a limited period of time, then persist or regress along with the age of the subject. We all have nevi and no problems. However, if melanocytes become capable of unlimited growth, to infiltrate adjacent tissues and to extend at distance (maligmant melanocytes), a melanoma arises. Therefore, melanoma is a malignant tumor composed of melanocytes; it may arise in all organs; in 99% of cases, however, it is a cutaneous neoplasm. It may be a flat or palpable lesion, sometimes a nodule; it is generally larger than 5 mm, asymmetric, with irregular borders, variegated in color with dark or black areas and whitish zones. It enlarges inexorably, can be ulcerated and bleeding. If the lesion is early detected, a patient with melanoma can be cured in 100% of cases. The survival rate decreases as the diagnosis is delayed. In the time, in fact, melanoma goes deeper and its thickness increases. The rate of survival of patients is as high as lower is the thickness of the tumor. Melanomas with a thickness lower than 1 mm (thin melanomas) carry a relatively good prognosis. The treatment of melanoma is surgical excision. Dematopathology must confirm that the excised lesion is a melanoma, because sometimes some nevi tend to simulate melanoma. Dermatopathology must also establish the thickness of the tumor (in millimiters and fractions). A parameter which presents analogies with the thickness is the level (of Clark), that is to establish what skin structures melamoma infiltrates (Level I = infiltration of the epidermis; level II = discontinous infiltration of the papillary dermis; level III = massive infiltration of the papillary dermis; level IV = infiltration of the deep (reticular) dermis; level V = infiltration of the subcutaneous fat). On these elements and others, therapy of melanoma is based.
The other pages
- Home Page: Dermatopathology - C. Urso, MD
- page 1: Melanoma of the skin
- page 2: Histologic diagnosis of cutaneous melanoma
- page 3: Melanoma arising in a melanocytic nevus
- page 4: Infiltration and pseudoinfiltration
- page 5: Sweat gland carcinomas
- page 6: The sentinel lymph node in cutaneous melanoma
- page 7: Bullous cutaneous diseases
- page 8: Spitz nevus
- page 9: Prognostic factors in cutaneous melanoma
- page 10: The dysplastic nevus
- page 11: Dermatofibrosarcoma protuberans
- page 12: Melanoma in situ
- last page: Questions, comments and opinions
page 13: Merkel cell carcinoma
page 14: Basal cell carcinoma
page 15: Melanoma in paediatric age